Back Surgery for Scoliosis

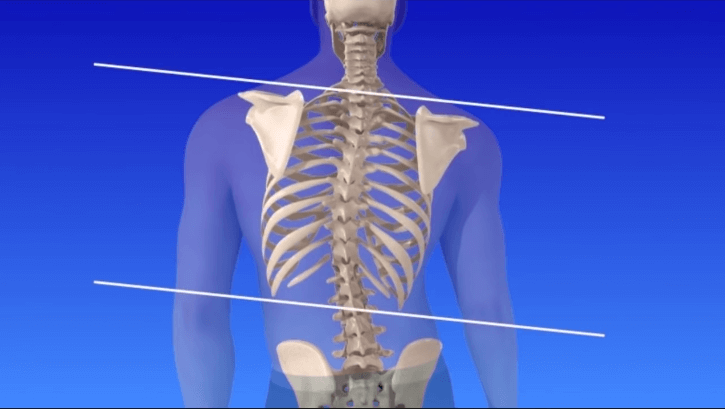
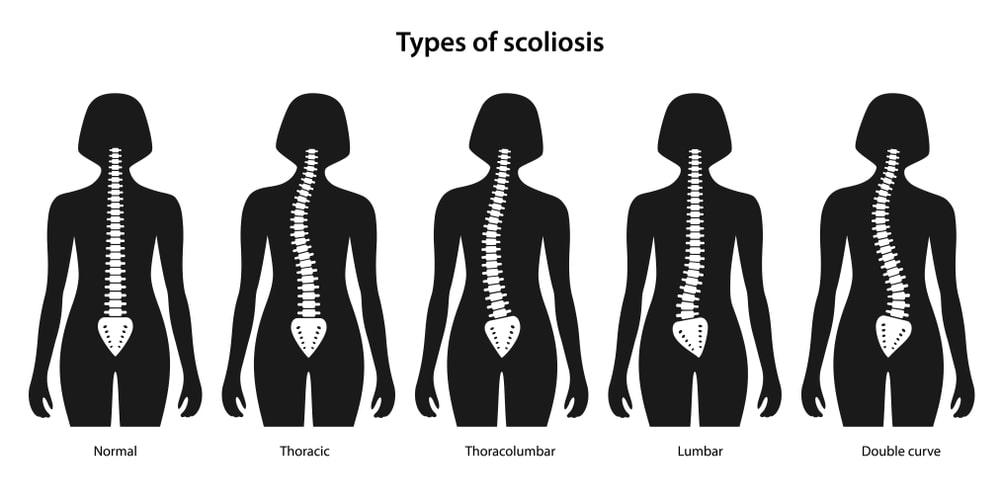
All of us have a natural curve to our spines, where it curves out at the neck, in at the thoracic area, and out again in the lumbar spine. These curves can become pronounced in conditions such as spondylolisthesis or ankylosing spondylitis, putting pressure on the spine and leading to further degeneration, deformity, and pain. Looking at the spine from the front or back should reveal no curves however, and scoliosis is a spinal condition that creates C-shaped or S-shaped curves where the spine should appear straight. These sideways curves may be quite subtle and cause few problems, but they can also cause pronounced curvature and lead to pain, dysfunctional movement, and difficulties with other normal physiological functioning such as breathing or digestion.
Scoliosis in Children
Scoliosis, referencing the Greek word meaning ‘crooked’, is often associated with children and adolescents, but it can affect adults too (normally due to going undetected in childhood). When young, a child with signs of scoliosis may be given a brace to wear to attempt non-surgical correction of the spine. This brace may help to encourage the spine to grow straight and for the structural ligaments, tendons, muscles, and bones in the back to create a more natural curve front to back, rather than side to side. For older children and adults this bracing is unlikely to be of much assistance other than support as the spine is usually fairly fixed in structure. Similarly, those with extreme abnormal curvature may find bracing ineffective and be advised to undergo back surgery more quickly. This can be especially frightening for younger children, as they can feel self-conscious due to the diagnosis and fearful of the operation itself. Early treatment is, however, very important as it gives the child a better chance at correcting the problem before it becomes too pronounced.

Problems Associated with Scoliosis
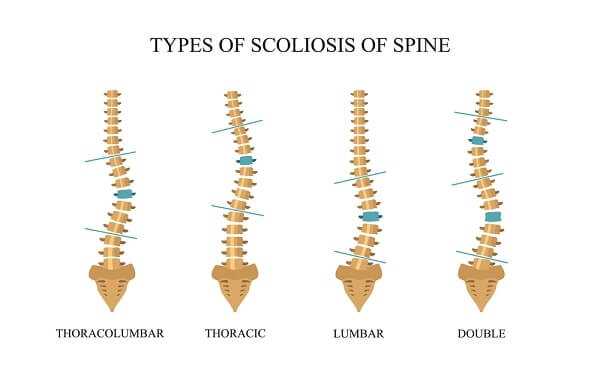
More pronounced spinal curvature with scoliosis can lead to problems with the cardiopulmonary system ad require more immediate surgery. Alternative techniques, such as ribcage expanders, may be appropriate in younger children. Most scoliotic curves occur in the thoracic spine and are treated through posterior spinal surgery using fusion techniques. Correction rates are usually around 50% for back surgery for scoliosis. For patients with curvature in the thoracolumbar region an anterior surgery may be the preferred option as more segmental motion may be retained in this procedure which can reduce later complications such as arthritis and pain development. Thoracoplasty alone, or in conjunction with either of these surgeries, involves the removal of ribs for bone grafting purposes or to correct a rib hump deformity. The ribs grow back, usually straight, in alignment with the corrected spine. As there are many potential courses of treatment for scoliosis, patients, and parents of younger patients with the condition are encouraged to discuss their options thoroughly and take time to make their decision as most cases do not require immediate action unlike some other spinal conditions where nerve function may be significantly compromised through treatment delays.
Symptoms of Scoliosis
Observing the signs and symptoms of scoliosis is not always easy, and parents may not notice the problem until it becomes significantly pronounced. A school nurse is often the first one to raise the issue, or parents may suddenly see a difference between their child and his/her sibling, or other children, when at a pool party or on the beach. Some signs to watch out for include uneven shoulder height, the whole body leaning to one side, and uneven rib cage or rib protrusion on one side. For a number of parents, the first sign of scoliosis is a clear disparity in the length of one trouser/pant leg indicating a hip imbalance, or scuffing on the bottom of one side of a pant-leg. Children may also complain of growing pains, back and/or leg pain, and abnormal fatigue, especially after long walks or other exercise.

Symptoms of Scoliosis in Adults
Adults can also experience scoliosis symptoms and may be less likely to consider them abnormal in light of a stressful job, other physical aches and pains, or learned habits. Spinal nerves are not usually compromised acutely by scoliosis, so symptoms of radiculopathy, paraesthesia, pain, numbness, and weakness are not considered indicative of scoliosis itself. The condition may, however, contribute to other spinal problems, especially in adulthood, which can cause such symptoms of nerve compression through disc degeneration, herniation, rupture, and bulging, or through joint hypertrophy or osteophyte growth.
Back surgery for scoliosis is often recommended for children if the curvature is likely to have a cosmetic effect in adulthood, has developed to more than 45-50 degrees of magnitude, is present alongside spina bifida and/or cerebral palsy, or affects physiological function such as breathing. Severe curvature or more than 50 degrees indicates a higher probability of the deformity progressing into adulthood. Spinal curvatures of 70-90 degrees will begin to restrict cardiopulmonary function in most patients as the space for the lungs and heart is closed down as the spine rotates the chest. Younger patients may be offered an alternative to scoliosis surgery which involves the use of a ribcage expander to allow more comfortable breathing and cardiac function whilst facilitating the straightened growth of the spine. The technique is fairly novel and, while it looks promising, has little in the way of evidence of efficacy or safety in the long-term.
Scoliosis Diagnosis
When diagnosis scoliosis and considering surgical treatments for a child, a physician may also order a renal sonogram and an electrocardiogram. This is because scoliosis as a congenital condition comes from a development issue in utero and may be present alongside defects in other organs or systems that develop at the same time. In the third to sixth week of pregnancy the heart and kidney systems are beginning to form and these tests can give an indication of possible problems that may prevent the child from undergoing surgery or need additional treatment.


Anterior Thoracolumbar Surgery for Scoliosis
For patients with a highly rigid curvature and a severe deformity, the surgeon may need to remove the disc from the front of the spine using an anterior approach. This can be an open incision or a minimally invasive surgery using a thorascope. Several discs may be removed in this procedure and bone grafts inserted into the disc space to restore the intervertebral height and facilitate the fusion of the vertebrae into one long piece of bone. If a young patient with a lot of growth left to occur has a posterior fusion alone then they can suffer from a complication known as ‘crankshafting’. This is where the front of the spine continues to grow in spite of the posterior fusion, causing an alteration in the posterior/anterior curvature. Anterior fusion prevents this complication from occurring and is a preferred technique in younger children.
Anterior Scoliosis Surgery
Back surgery for scoliosis utilizing the anterior method may also be preferred where the curvature exists mainly in the thoracolumbar region, specifically at T12-L1. The surgeon will make an incision in the lower chest and remove a rib (generally from the left side) to obtain access to the anterior spine. The discs are excised which reduces the rigidity of the spine, and screws are affixed to the vertebrae to be connected by a metal rod which provides the curvature correction. The surgeon then inserts the bone graft for fusion into the disc space and may use further instrumentation to hold it in place. The formation of a solid fusion can take between three and six months, and continues for up to twelve months in some patients. Regularly x-rays will be conducted to assess the success of the operation and to catch any potential complications early. Irritation of the surrounding tissues by the rod used for curvature correction is not common, but can occur, leading to the removal of the rod once fusion has occurred.
Anterior scoliosis surgery has the advantage of generally requiring the involvement of less vertebral levels, thereby maintaining a higher degree of segmental motion in the spine. In the lumbar spine this can be particularly helpful in reducing the risk of arthritis development which is more likely with fusion below the L3 vertebral level. Anterior surgery for scoliosis can provide excellent cosmetic results an better reduction in curvature, but is only appropriate for the thoracolumbar region. Most scoliosis is present in the thoracic spine however, which requires alternative, posterior fusion surgery.
Posterior Spinal Fusion for Scoliosis
Back surgery for scoliosis is primarily in the form of spinal fusion with instrumentation. The bone graft used may be autologous, and is harvested from the patient’s hipbone during the spinal surgery. An autograft such as this is considered the best option for most patients in order to encourage a solid fusion, but where the secondary operation is contraindicated the surgeon may use donated cadaverous bone instead, or new types of synthetic graft material. Spinal fusion aims to prevent worsening of the curve and to provide some degree of correction to the existing curvature. The spinal fusion will cause some rigidity in the spine, however, and restricts certain movements and flexibility as some of the vertebrae are fused into one long bone rather than separate, movable, segments.
New Techniques for Scoliosis Surgery
The advent of metal instrumentation made a significant difference in the success of spinal fusion surgery for scoliosis. Originally the patient had no instrumentation inserted but was placed in a cast after surgery to hold the spine straight while fusion occurred. This often led to failed fusion (pseudoarthrosis) and contributed to further spinal problems due to lengthy bed rest causing muscle atrophy in the back. The methods of traction used in attempts to straighten the spine often led to increased wear and tear, osteoarthritis at an early age, disc degeneration, and heavy dependence on pain medications into adulthood. Patients were often diagnosed with ‘Flatback’ as a complication of lumbar scoliosis surgery, and were frequently unable to work or experience reasonable quality of life.
Luckily, modern back surgery techniques have addressed many of these problems, and scoliosis surgery is often extremely effective at reducing patients’ symptoms and improving their quality of life. Combinations of rods, plates, screws, hooks, and wires implanted during surgery can effectively counter the sagittal (sideways) imbalance, and the rotational dysfunction of scoliosis. The newer technique is known as the Cotrel-Dubousset instrumentation, in contrast to the old …. Rod technique. The newer surgical technique appears very effective at restoring normal function in younger children and has shown little in the way of complication. Unfortunately, due to the recency of back surgery developments for scoliosis, few patients are available as examples of how the spinal surgery progresses into adulthood.
A comparison of the old and new techniques in patients with adolescent idiopathic scoliosis (AIS) found that the use of pedicle screws alone in a posterior spinal fusion facilitated a major curve correction in 65% of patients compared to the 46% in the surgeries using pedicle screws and proximal hooks (Kim, et al, 2006). The retrospective, versus prospective, review of the cases may contribute to bias in this data analysis, but the results do seem to be supported by the experiences of other spinal surgeons working in this field.
Scoliosis Surgery Recovery
Scoliosis surgery recovery period depends largely on the exact procedure carried out. For more invasive surgeries the patient will usually spend around four days to a week in a hospital and can start to move around after around two or three days. School students are usually able to return to class after two to four weeks but are restricted in some activities as the bones continue to fuse. A brace of restrictive device may need to be worn on occasion, particularly in the first few days and weeks, to prevent sudden movements of the spine from affecting the formation of a solid fusion. Bending, lifting, and twisting can all upset the hardware used during fusion back surgery and may result in a pseudoarthrosis; these activities are generally restricted for the first three months or so after back surgery for scoliosis.
Avoiding High Impact Sports
High impact sports, such as running, and contact sports, such as football or wrestling, are discouraged for around six months to a year after surgery as they can severely compromise fusion success. Any other physically jarring or jolting activities are also to be restricted, which can be difficult to monitor in children. Parents should ensure that their child’s teachers and friends are aware of the surgery and its connotations so that their child is not pressured into activities which may compromise recovery and surgical success. Patients who have had a thoracolumbar fusion procedure may be able to resume activities more quickly as this operation does not significantly affect the biomechanics of the spine. Obtaining specific activity guidance from the surgeon is extremely important.
Monitoring the Progress of Scoliosis Surgery
X-Rays and other diagnostic imaging and physical checks are used to monitor patients for one to two years after scoliosis surgery. Evidence of a solid fusion usually means that no further treatment is necessary in the immediate to mid-term. Women who undergo scoliosis fusion should have no complications as regards conceiving and giving birth vaginally after the operation. Most women experience some degree of lower back pain during pregnancy, but this should be addressed with a physician if the patient is concerned at all.
Scoliosis Surgery Risks
Back surgery for scoliosis is indicated in around 5% of cases and patients, and the parents of younger children with scoliosis, need to consider the possible complications of back surgery. Inflammation, infection, breathing problems, blood loss, and potential nerve injury are all risks associated with back surgery for scoliosis. Some patients will be more at risk than others, those who are overweight for example, smokers, and those with other compromising medical conditions such as diabetes or respiratory issues. The possible need for additional back surgery is also a major consideration when deciding on scoliosis surgery. A number of patients (around 5%) require additional surgery after just five years, and the modern techniques have not had time to establish a longer-term prognosis. The necessity of surgery based purely on cosmetic reasons remains open to interpretation, with many surgeons hesitant to perform such invasive procedures without a physiological impairment (such as respiratory complication) present.
Correction Rates for Scoliosis Surgery
Scoliosis is rarely corrected completely, but back surgery can make a significant difference to daily pain, discomfort, and self-consciousness about the appearance. Corrections rates are usually around 50% for spinal fusion surgery. The surgery itself is usually through anterior or posterior spinal fusion, depending on the site and degree of curvature. In some cases, both types of surgery are conducted during the same procedure or two separate procedures, with surgery for scoliosis often taking four to eight hours and having a significant period of recovery and rehabilitation afterwards. The incision made during back surgery for scoliosis usually runs the full length of the spine.
Risks of Paraplegia
There is a risk of paraplegia with surgery for scoliosis, although this is extremely rare and has around a 1/1000-1/10,000 chance of occurring. Some surgeons make use of somatosensory evoked potentials, and motor evoked potentials to monitor nerve signalling during the surgery. Other surgeons may use a Stagnara wake up test involving waking the patient and asking them to move their feet during the surgery. The patient does not remember being woken after surgery, and does not feel any pain during this brief period of consciousness. If nerve function appears compromised then the surgeon can cut the rods and abandon the surgery in order to reduce the risks of paraplegia. The patient will then be tested to ensure neurological function is intact and surgery can be rescheduled.
Blood Loss Durgery Scoliosis Surgery
Blood loss is a major risk during scoliosis surgery as the patient has a significant degree of muscle tissue stripped or cut during the procedures. Some surgeons ask for the patient to donate blood prior to surgery in order to be prepared for any necessary transfusion in the procedure itself. It is also possible to collect and transfuse the patients’ blood that is lost during surgery in some cases. Infection, both deep and shallow, can occur after surgery and has an incidence of around 1%, hardware failure is extremely unlikely, but remains a possibility, as does nerve damage and allergic reaction to the anaesthesia. Failure of spinal fusion to occur presents, perhaps, the highest risk, with around 1-5% of patients not achieving a successful fusion of bone.
Alternatives to spinal fusion for scoliosis do exist, with the main intention of delaying the need for fusion surgery and allowing children to grow whilst addressing some possible complications due to their scoliosis. Implants in the ribcage can help smaller children with breathing difficulties and cardiac pressure by pushing the ribs apart on the compressed side. Vertical expandable prosthetic titanium ribs (VEPTR) can successfully expand the child’s chest cavity to allow more comfortable breathing whilst exerting a straightening effect on the spine as the child continues to grow. The flexibility of the spine is, therefore, maintained due to the non-use of fusion. The VEPTR technique is only appropriate in a growing child, and is a novel operation with little in the way of long-term outcomes.