What Do I Do If My Surgery Doesn’t Seem to Have Worked?

Occasionally, surgery for back problems doesn’t work out the way it was intended. This has been called failed back surgery syndrome by some doctors and other people not familiar with the true issues. There are many reasons why surgery results are not always ideal. If you are a back patient whose surgery didn’t work, the key issue is finding out why.

Reasons That Back Surgery Can Fail
1. A back problem could be misdiagnosed or incompletely diagnosed. All good back treatment, especially surgery, depends on getting a good diagnosis. Surgery works best when the surgeon understands exactly what is wrong with your back and how to fix it. Unfortunately, sometimes the true source of a patient’s pain is misdiagnosed. In this case, the surgeon thinks the patient’s pain is coming from one problem when it is actually due to a different problem. For example, Dr. Winter recently saw a case at a conference in which a patient had severe leg pain and an MRI that showed a disc bulge. The logical conclusion was that the disc bulge was pinching a nerve, thus causing the leg pain. The patient was scheduled for surgery to remove the disc bulge. At surgery, the nerve was swollen and irritated, but it was not compressed by the disc. Two days later, the patient exhibited shingles, a viral infection involving the nerves. This infection was causing the leg pain.
Another example of misdiagnosis is a patient with a herniated disc who is operated on at the wrong level. In this case, the operation should be performed again at the correct level, probably by a different surgeon.
If a back problem is incompletely diagnosed, surgery might help but may not completely fix the problem. For example, if a patient had surgery for a disc herniation with both back and leg pain and got good relief from the leg pain but continues to have major back pain, it is probably because the disc that was ruptured was also degenerated. The surgical answer is not another discectomy but rather to treat the degeneration with fusion surgery (or perhaps in the future with disc replacement surgery).
A similar situation can occur after decompression surgery for spinal stenosis. Nerve compression symptoms (pain, weakness, and/or numbness in the legs) may go away, yet increasing back pain occurs. This is caused by degeneration of the discs, not stenosis. If the pain is bad enough, the patient might need a second surgery—a fusion operation—to fix the degeneration. This is not a problem due to misdiagnosis, since the surgeon knew of the degeneration and hoped that the decompression would also help the back pain (which it often does). The surgeon wanted to spare the patient the additional trauma of a fusion operation.
2. The correct surgical procedure could be incompletely performed. Sometimes the surgeon will know exactly what is wrong and perform the correct surgery, but the patient will still have pain.
This may happen if the surgical procedure was not done thoroughly. For example, the patient might have decompression surgery for a pinched nerve (or nerves) in her back. If the decompression is not fully accomplished—that is, if whatever is pinching the nerve(s) is not cleaned out completely—the pinching may continue. In this case, a repeat laminectomy may be necessary after tests are done to confirm the problem.
3. A person may not respond well to surgery. Your body must respond to surgery in a predictable, healthy manner in order for it to be successful. This is particularly important for fusion surgery. The goal of any fusion surgery is to have two bones solidly fuse together. When a fusion fails and the two bones do not heal properly, it is called a pseudarthrosis (pseudo means “false” and arthrosis means “joint”). This is usually but not always a painful situation.
A fusion operation may fail to work or fuse for many reasons. Smoking, anemia (low blood count), diabetes, obesity, and inactivity have all been shown to hinder fusion healing.
If a patient has had a nonhealing fusion operation, the only way to eliminate the pain is to do further surgery to achieve a solid union of the two bones. It has been shown that going back into the old incision and just adding more bone graft often doesn’t work. Better results are achieved by going in and doing more complex surgical work.
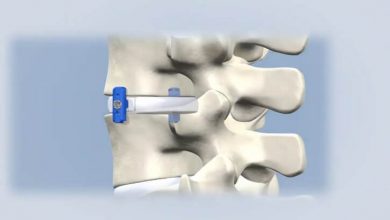
If a patient has had a typical lower back posterior fusion without instrumentation, the best results will probably come from adding an anterior interbody fusion plus redoing the posterior fusion and adding instrumentation. If a patient has had a typical lower back posterior fusion with instrumentation, the best results will probably come from adding an anterior interbody fusion, plus rechecking the posterior fusion, adding more bone graft, and tightening up the instrumentation or replacing it.
If a patient has had an anterior interbody fusion with a cage, the best results will probably come from redoing the anterior fusion with cage removal, adding bone graft anteriorly, then doing a posterior fusion with instrumentation. If a patient has had a thoracic scoliosis operation and a pseudarthrosis has been found, the best results will probably come from a posterior reoperation with more bone graft and replacement of the instrumentation. If a patient has had a posterior-only operation for a kyphosis problem and has a pseudarthrosis, then the best answer is adding an anterior fusion plus redoing the posterior operation.
4. A back problem may reoccur either in the same place or in a different place. Sometimes surgery successfully treats a patient’s back problem, and a year or so later the pain comes back. If a patient had surgery for a disc herniation, this may mean the same disc has herniated again or a new herniation has occurred at another level. In either case, an MRI or CT myelogram will indicate the cause of the patient’s pain, and a repeat surgery may be necessary.
Spinal stenosis is another problem that can come back in a different place. A patient may have had decompression surgery and done well for one to five years only to have the nerve compression symptoms come back. This is almost always due to a new compression occurring at a place in the spine that was just fine at the time of the earlier surgery.
Dr. Winter’s secretary had a successful operation for spinal stenosis and degenerative disc disease (decompression and fusion). Five years later, her pain came back. Tests revealed that she had the same problem as before but in a different place. She had the same surgery done for the new problem and is doing just fine.
5. Surgery may cause a secondary problem. If screws and/or rods are used for a fusion operation, they can cause a localized irritation where the muscles rub over them. This is rare and can usually be solved be removing the screws and/or rods that are causing the problem.
The Next Step
If you had spine surgery but continue to have a lot of pain, an evaluation by a good spine surgeon is your next step. This doctor will likely be able to tell you why you continue to hurt and whether further surgery might help. You should begin, of course, with your original surgeon, since the answer and treatment may be obvious. If, however, your original surgeon says that everything possible has been done and you’ll just have to live with the pain, you must get another opinion from a good spine surgeon.
A good friend of mine (Dr. Winter’s), a young resident physician, had two failed back surgeries (laminectomies). She was so miserable and needed so much pain medication that she could not perform her duties as a resident doctor. She was told by her neurosurgeon that everything possible had been done. She got a second opinion from a good spine surgeon, was properly diagnosed, and underwent appropriate fusion surgery. Now, five years later, she is completely pain-free and working full-time as a physician. She calls her decision to seek another opinion and have further surgery “the best decision of my life.”
Don’t adopt a nothing-more-can-be-done mindset. Seek another opinion! It is hard to see people chronically addicted to pain medications when their problem could be fixed.
There might not be a surgical answer to your problem. If that is true, your doctor can help you find the best solution for your situation. As we discussed in this article, our minds can powerfully affect how we heal and how much pain we have. Psychotherapy can help if the doctor determines that most of your pain is caused by errant mental or emotional processes.
You may have a back problem that cannot be repaired with further surgery. Psychotherapy can help you learn strategies for living with your pain. In addition, narcotic medication, an implanted spinal cord stimulator, or a morphine pump can be used to treat pain.
Finally, there may be a surgical answer to your problem, but you may decide you don’t want surgery again. In this case, your doctor can help you make the best of your situation with pain medications, pain-control devices (such as a morphine pump), a referral to a chronic pain clinic, or a referral to psychotherapy.